 After a chaotic start to my travels with a 4-hour delay in Vancouver resulting in less than one hour to make a connection to Johannesburg in London (which our bags did not), I (Paul) have returned to the blog. Those who have been avidly following along will recall that this is my third sojourn to Karanda Mission Hospital, now 2 & 1/2 years since Lori, Rachelle and Thea were here. This time I linked up with the team that Dr Ray Markham puts together annually to visit Zimbabwe. It was Ray and his office staff who initially installed the electronic medical record (EMR) Medical Office Information System (MOIS) at Karanda, at the request of their administration. My first visit in 2015 was inspired by a slide presentation I heard Ray give at a conference in Montreal and he had then encouraged me to continue the MOIS install.
After a chaotic start to my travels with a 4-hour delay in Vancouver resulting in less than one hour to make a connection to Johannesburg in London (which our bags did not), I (Paul) have returned to the blog. Those who have been avidly following along will recall that this is my third sojourn to Karanda Mission Hospital, now 2 & 1/2 years since Lori, Rachelle and Thea were here. This time I linked up with the team that Dr Ray Markham puts together annually to visit Zimbabwe. It was Ray and his office staff who initially installed the electronic medical record (EMR) Medical Office Information System (MOIS) at Karanda, at the request of their administration. My first visit in 2015 was inspired by a slide presentation I heard Ray give at a conference in Montreal and he had then encouraged me to continue the MOIS install.
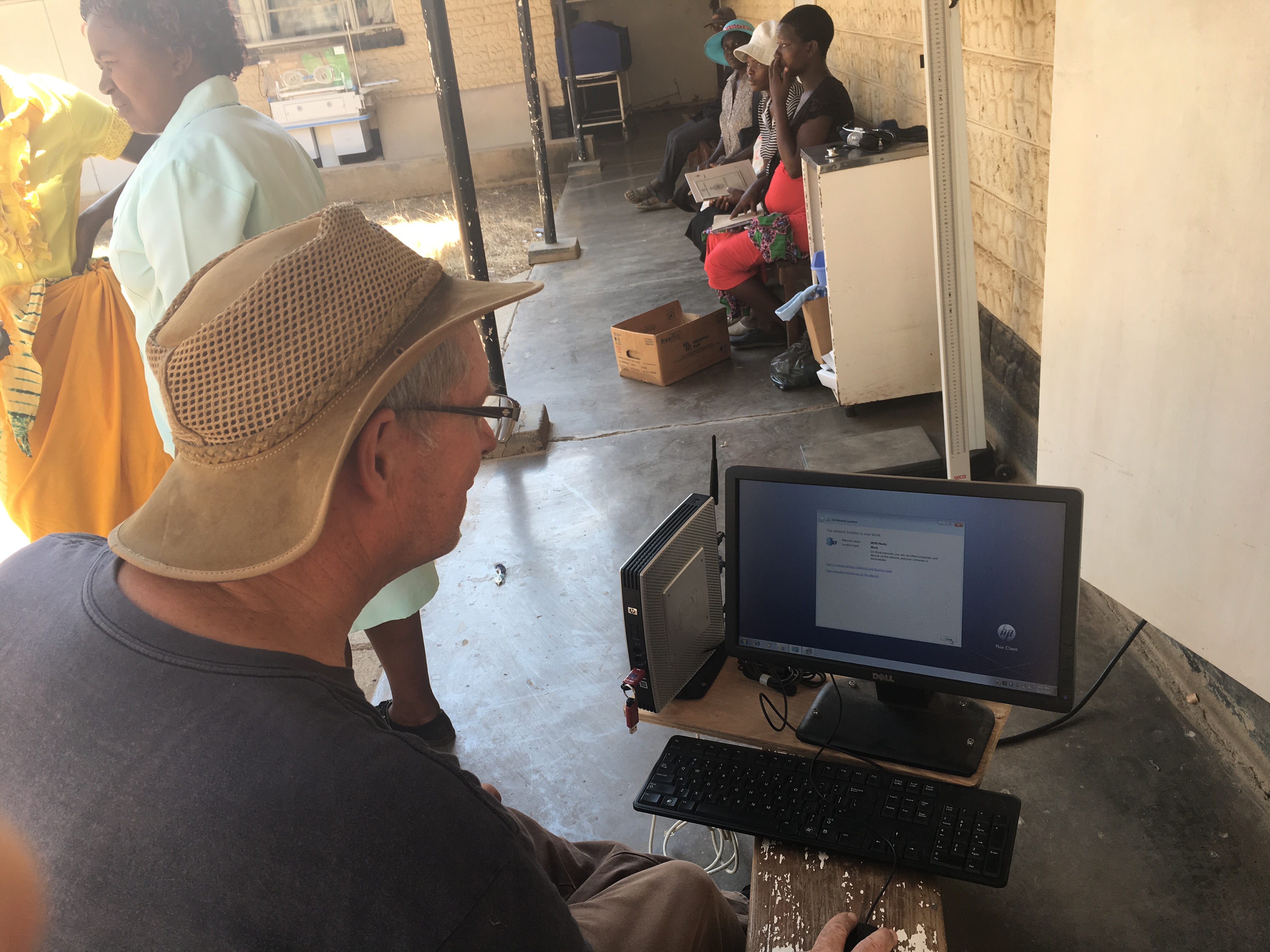
I always have some trepidation when encouraging others to embrace computer technology in their work (particularly healthcare) as I am fully aware that it takes immense time and effort for people, especially those on the front lines here who are extremely busy. Thus each time I have returned to Karanda I am curious to see how much training has been retained and which features of the system are still being used given the demands of working here, not the least being the erratic power supply.
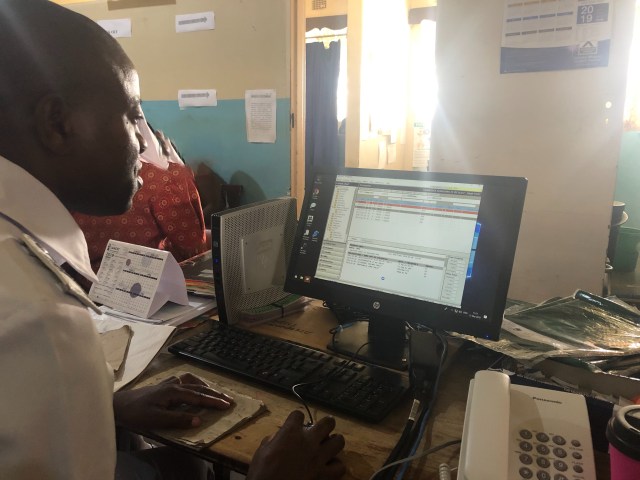 Once again the staff of Karanda have excelled. Some may recall that most of our efforts last time were to try and remove the need for the multiple accounting ledgers that were being used to record information, which some staff member then had to trawl through to extract the data required by the Zimbabwe Ministry of Health. Thus it was particularly gratifying to see that each department with MOIS was still “off book” except for the subset that the Ministry requires in a particular ledger (essentially HIV and TB). It was also incredibly gratifying to see the rapid and almost effortless way the staff were then able to extract the data they needed to (in a minute or two versus hours). Well almost effortless as there was a tiny (but extremely annoying) bug because of Canada being “Letter” and Zimbabwe being “A4” for printers. However after a few hours of: “I should remember how I fixed this!!” I did indeed remember.
Once again the staff of Karanda have excelled. Some may recall that most of our efforts last time were to try and remove the need for the multiple accounting ledgers that were being used to record information, which some staff member then had to trawl through to extract the data required by the Zimbabwe Ministry of Health. Thus it was particularly gratifying to see that each department with MOIS was still “off book” except for the subset that the Ministry requires in a particular ledger (essentially HIV and TB). It was also incredibly gratifying to see the rapid and almost effortless way the staff were then able to extract the data they needed to (in a minute or two versus hours). Well almost effortless as there was a tiny (but extremely annoying) bug because of Canada being “Letter” and Zimbabwe being “A4” for printers. However after a few hours of: “I should remember how I fixed this!!” I did indeed remember.
It was also heartening to see how the staff adapted some of the workflows I had started. In some cases, they figured out that my way wasn’t working and so they came up with a better, simpler way. As usual everyone greeted me very warmly and generously, despite me being the “MOIS doctor”. It has been wonderful reconnecting with people and they are very patiently re-teaching me all the Shona I had forgotten.
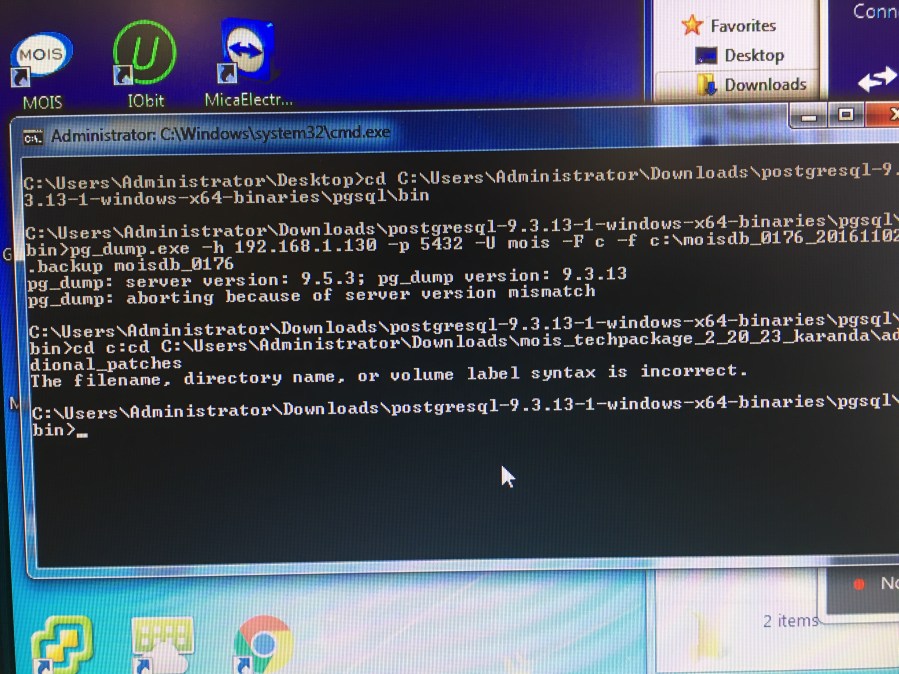
Of course there have also been some hiccups. During this visit, we updated MOIS and, as expected, the update “broke” a few of my workarounds. Nothing I wasn’t expecting and the update now gives me the tools to do the local adaptations properly. However it does mean the keyboard grunt work has to be done. I do have the luxury of doing this in the computer room which is air-conditioned, unlike the other hospital departments and wards. As before, MOIS staff back in Prince George have endured my numerous requests and given me solutions.
 This time of year is the rainy season and therefore “cooler” than the 40 degrees we all experienced in Oct 2016. However the fans are still required in the day and are missed when the power goes out. It does get a fraction cooler at night and I commented that this time was the first (on one night) that I actually had to pull up the bed cover. The difference in the vegetation is fascinating to see after the rain, with everything that was brown before now green. However the rains have been less than usual and the season appears to have finished early, which does not augur well for the coming dry. Already the water is being turned off at various times.
This time of year is the rainy season and therefore “cooler” than the 40 degrees we all experienced in Oct 2016. However the fans are still required in the day and are missed when the power goes out. It does get a fraction cooler at night and I commented that this time was the first (on one night) that I actually had to pull up the bed cover. The difference in the vegetation is fascinating to see after the rain, with everything that was brown before now green. However the rains have been less than usual and the season appears to have finished early, which does not augur well for the coming dry. Already the water is being turned off at various times.
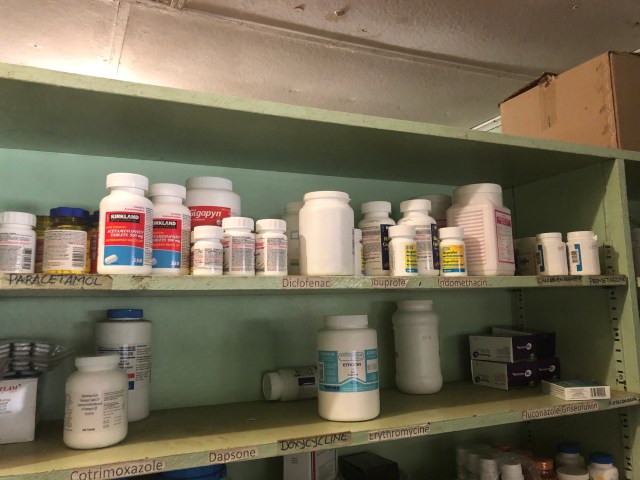
Because of rising prices, the hospital has even fewer medications available than before. For this trip, Lori arranged a substantial supply of medications through Health Partners International of Canada (HPIC). Something as basic but as essential as acetaminophen was being rationed before our arrival and the various antibiotics in the HPIC boxes were particularly appreciated.
Tania Bell, a wound and ostomy care nurse at Fort St John Pharmacy and Wellness Centre, joined me on this trip. She is very much in demand. As the Canadian Dr Thistle who works at Karanda full-time says of Karanda, ‘Pus Is Us’. Tania has been organizing all the donated dressings, developing simple protocols so nurses know how and when to use them, and teaching the nurses. She has also been adapting some of the wound-cleaning procedures. The staff at uniPharm, the wholesale company in Vancouver that supplies medications to various pharmacies throughout BC, generously donated many supplies such as eye patches, knee braces, etc. that were gratefully received.
 Amidst all these challenges to provide the basics it does seem a little irrelevant to be maintaining computers and printers and training people to use software. However the staff continue to be gracious and hard working and receptive to change. Ray always emphasizes capacity building on these trips and that is our goal. I have more “help” from Ray’s team arriving this week to expand the training, which staff have identified they need. I anticipate a productive week.
Amidst all these challenges to provide the basics it does seem a little irrelevant to be maintaining computers and printers and training people to use software. However the staff continue to be gracious and hard working and receptive to change. Ray always emphasizes capacity building on these trips and that is our goal. I have more “help” from Ray’s team arriving this week to expand the training, which staff have identified they need. I anticipate a productive week.
Maitabasa