The INTERNATIONAL JOURNAL of MACKEY MUSINGS
2023; 1(1): 1-6
12-Month Review of Two Middle-Aged Adults Yields Few Insights
Bonertz LM1,2,3, Mackey PV1,4,5,6.

Affiliations
1. Home, Kamloops, BC
2. Fort St John Pharmacy, Fort St John, BC
3. Tumbler Ridge Pharmacy, Tumbler Ridge, BC
4. Apex Surgical Centre for Oral & Facial Surgery, Kamloops, BC
5. Cariboo Memorial Hospital, Williams Lake, BC
6. GM Baker Hospital, Quesnel, BC.
Conflict of interest statement
Lori would like to be sponsored by Hawkins Cheezies but to date no samples or branded clothing has arrived. Paul would like to be sponsored by Les Paul or Rocky Mountain Cycles to cover the purchase of more musical instruments or another bike.
Abstract
This 12-month, multi-centre, retrospective review reports on the low points and highlights of the Mackey family in 2023. Trends suggest skiing, hiking, mountain biking, paddling, hanging out with friends and family, and attending musical events provide much joy.
Key words: skiing; hiking; family; friends; healthcare
Introduction
The authors struggled to devise a novel theme for this year’s Christmas letter. Because they participated in a BCCDC Sentinel Household Surveillance Network 1 and Paul is now enrolled in the PATRON study2, a review article seemed the most appropriate.
Methods
A random survey of photos and memories collected by the authors over the past 12 months was conducted. A limited search of MEDLINE was performed to survey the current literature. No demographic data was collected, and no statistical analyses were performed.
Results
Low points
In April, Paul underwent a radical prostatectomy for prostate cancer. We found it rather surreal for him to be a patient in the Royal Inland Hospital where we met in 1989, esp. as the surgical ward has not altered much since Paul was there briefly as a medical student and Lori worked as a hospital pharmacist. Paul’s post-surgical recovery was mostly smooth (much of it spent in his TARDIS housecoat) (Fig. 1). However, he also had to undergo radiotherapy, which entailed being in Kelowna weekdays beginning Nov. 29 (and will continue to January 10).

Wildfires were widespread across BC, beginning north of Fort St John early in the season and affecting almost every part of the province by summer’s end. Air quality was often poor and friends in various regions were affected by evacuation alerts or actually forced to evacuate at times.
Our cat, Pepsi, acquired from the Pimms in 2008, died in August after a short illness and we still find ourselves checking to see whether he needs to be fed or let in the house.
Highlights
The conditions during the 2022–23 ski season were superb, both for downhill and cross-country skiing. Our skate-skiing technique still needs improvement and Paul had an encounter with Nancy Greene3 on a black downhill run that left him feeling humbled, but we both appreciated our ready access to Stake Lake trails and Sun Peaks4 (Figs 2,3).



Most of our kids and Lori’s sister Michele and her kids Lara and Aleks joined us at Sun Peaks after Christmas 2022. We also had the chance to ski at Revelstoke with a mix of Mackeys that included two of Paul’s cousins (David and Patrick, two of Patrick’s children (Lucie and Apie), our sister-in-law Melissa, and her daughter Lexie (Fig. 4). In March, Paul was able to meet Jeryn and Ted in Jasper for spring skiing.
Our friend Michelle travelled to Canada in May. We had some time to just hang out as well as do some amazing hikes (Fig. 5). We also tested the utility of having your own experienced rural physician travelling with you when one (Paul) dislocates one’s shoulder 2 hours from a medical facility.

In 2013, the year of our 20th anniversary, our friends Becky and Leo had met up with us in NYC and they were able to join us there again, 10 years later. (Fig. 6). Michelle rounded out our quintet. Paul sang at Carnegie Hall (Fig. 7) with the choir from Kamloops and we went to several musicals (including Sweeney Todd featuring Josh Groban), an outdoor production of Hamlet in Central Park, and various museums.


In July, we travelled to Melbourne to spend time with Paul’s Dad and Sandra and see other friends and family. The light show at the botanical gardens was a bonus, Paul got to see Collingwood win a match, and we dined in the Member’s at the MCG before a Demons match, which they conveniently won for Paul’s Dad’s benefit. (Fig. 8). Of course, Paul was very pleased that Collingwood won the Grand Final in September.5

In August, we drove to Pincher Creek for Lori’s 40-year high school reunion. There was a solid turnout from our small class, including some parents, teachers, and siblings, and the reminiscing was entertaining. We caught up with family, stayed one night with friends in Waterton, and hiked the trail to Crypt Lake with Lori’s friend Angela (Lori overcoming her fear of heights to negotiate the chain and tunnel section). (Fig. 9)

In November, Paul made a quick trip to California to meet up with David for some hiking and touring around. (Fig. 10)
This year, we hosted three indoor house concerts (Rachel Casponi, Naomi Shore, Danny Bell). Our listening adventures were rounded out by a Frank Turner concert and a Bryan Adams concert plus various Kamloops Chamber Musicians and Kamloops Symphony Orchestra concerts.
Paul got out mountain biking whenever he could, often joining the local group rides. Lori really enjoys the year-round Friday morning running group. We checked out known and new-to-us lakes for kayaking and stand-up paddle boarding.


Paul continues to do rural family practice/anesthesia locums, mostly in BC, as well as anesthesia for a dental surgeon, and some family practice and teaching family practice residents in Kamloops. Lori helps out when she can at the pharmacies in Fort St John, Keremeos, Tumbler Ridge, and West Kelowna; administers vaccines in assisted-living facilities; and edits medical manuscripts (until she is replaced by ChatGPT). The changes in practice that allow pharmacists some prescribing authority have added to the workload but also to the work satisfaction.
Our kids are forging their various paths: Jeryn and Ted up in Fort St John, Liam and Rachel relocating to BC (Fig. 11), Rachelle in Environmental Studies at Douglas College in Vancouver, and Anthea in third-year biology at the University of Alberta in Edmonton.
We are looking forward to Paul’s brother Simon and Melissa and their daughters joining us for Christmas.
Conclusion
The year 2023 offered challenges not previously encountered as well as some fulfilling work, inspiring travel, connection with family and friends, wonderful music experiences, and opportunities for outdoor activity. Further research is needed to determine whether these trends persist and what the future holds.
We wish friends and family both near and far a happy Christmas and a joyful New Year.
References
1. https://covid19.research.ubc.ca/research/characterizing-antibody-response-emerging-covid-19-virus-care-covid-19 accessed Oct 21, 2023
2.Menard C, Young S, Zukotynski K, et al. PSMA PET/CT guided intensification of therapy in patients at risk of advanced prostate cancer (PATRON): a pragmatic phase III randomized controlled trial. BMC Cancer 2022;22(1):251.
3. https://en.wikipedia.org/wiki/Nancy_Greene_Raine accessed Dec 4, 2023
4. Spiteri K, Broom D, Laventure B, et al. Barriers and Motivators of Physical Activity Participation in Middle-Aged and Older Adults—A Systematic Review. J Aging Phys Act 2019;27(4):929-44.
5. https://studyfinds.org/i-love-you-happiness-sports/ accessed Oct 13, 2023
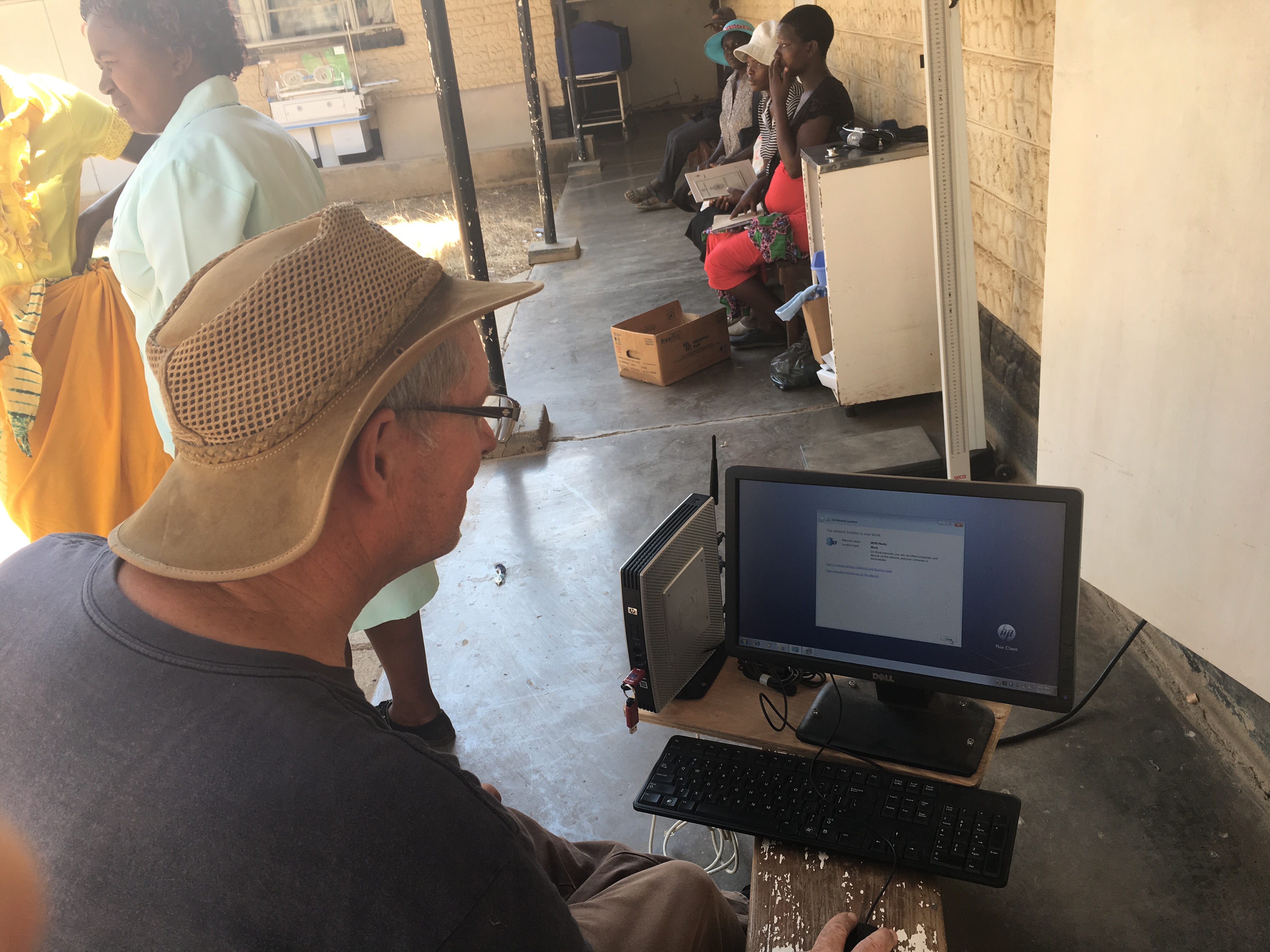
 After a chaotic start to my travels with a 4-hour delay in Vancouver resulting in less than one hour to make a connection to Johannesburg in London (which our bags did not), I (Paul) have returned to the blog. Those who have been avidly following along will recall that this is my third sojourn to Karanda Mission Hospital, now 2 & 1/2 years since Lori, Rachelle and Thea were here. This time I linked up with the team that Dr Ray Markham puts together annually to visit Zimbabwe. It was Ray and his office staff who initially installed the electronic medical record (EMR) Medical Office Information System (MOIS) at Karanda, at the request of their administration. My first visit in 2015 was inspired by a slide presentation I heard Ray give at a conference in Montreal and he had then encouraged me to continue the MOIS install.
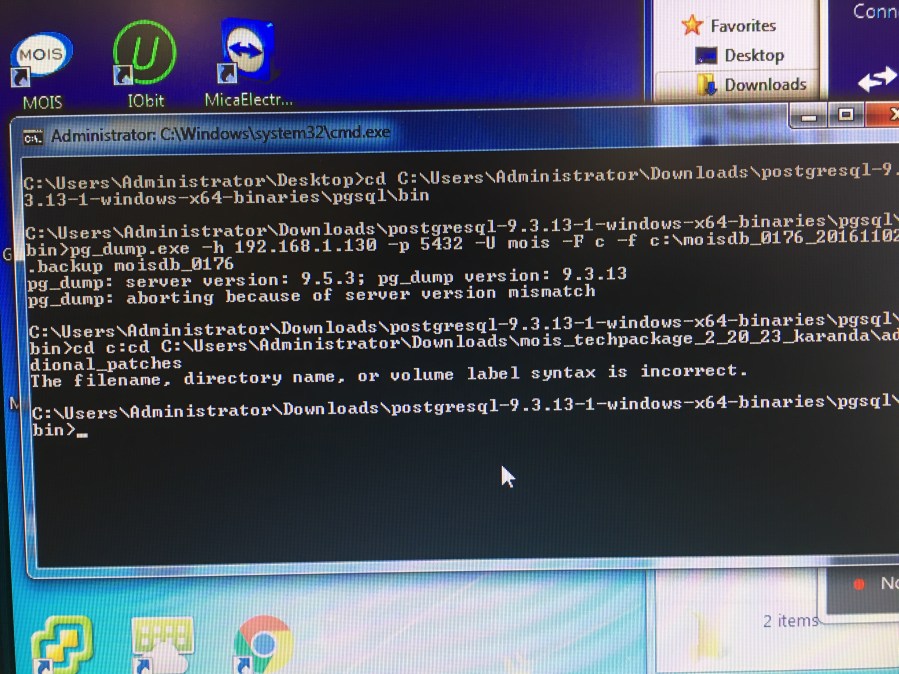
After a chaotic start to my travels with a 4-hour delay in Vancouver resulting in less than one hour to make a connection to Johannesburg in London (which our bags did not), I (Paul) have returned to the blog. Those who have been avidly following along will recall that this is my third sojourn to Karanda Mission Hospital, now 2 & 1/2 years since Lori, Rachelle and Thea were here. This time I linked up with the team that Dr Ray Markham puts together annually to visit Zimbabwe. It was Ray and his office staff who initially installed the electronic medical record (EMR) Medical Office Information System (MOIS) at Karanda, at the request of their administration. My first visit in 2015 was inspired by a slide presentation I heard Ray give at a conference in Montreal and he had then encouraged me to continue the MOIS install.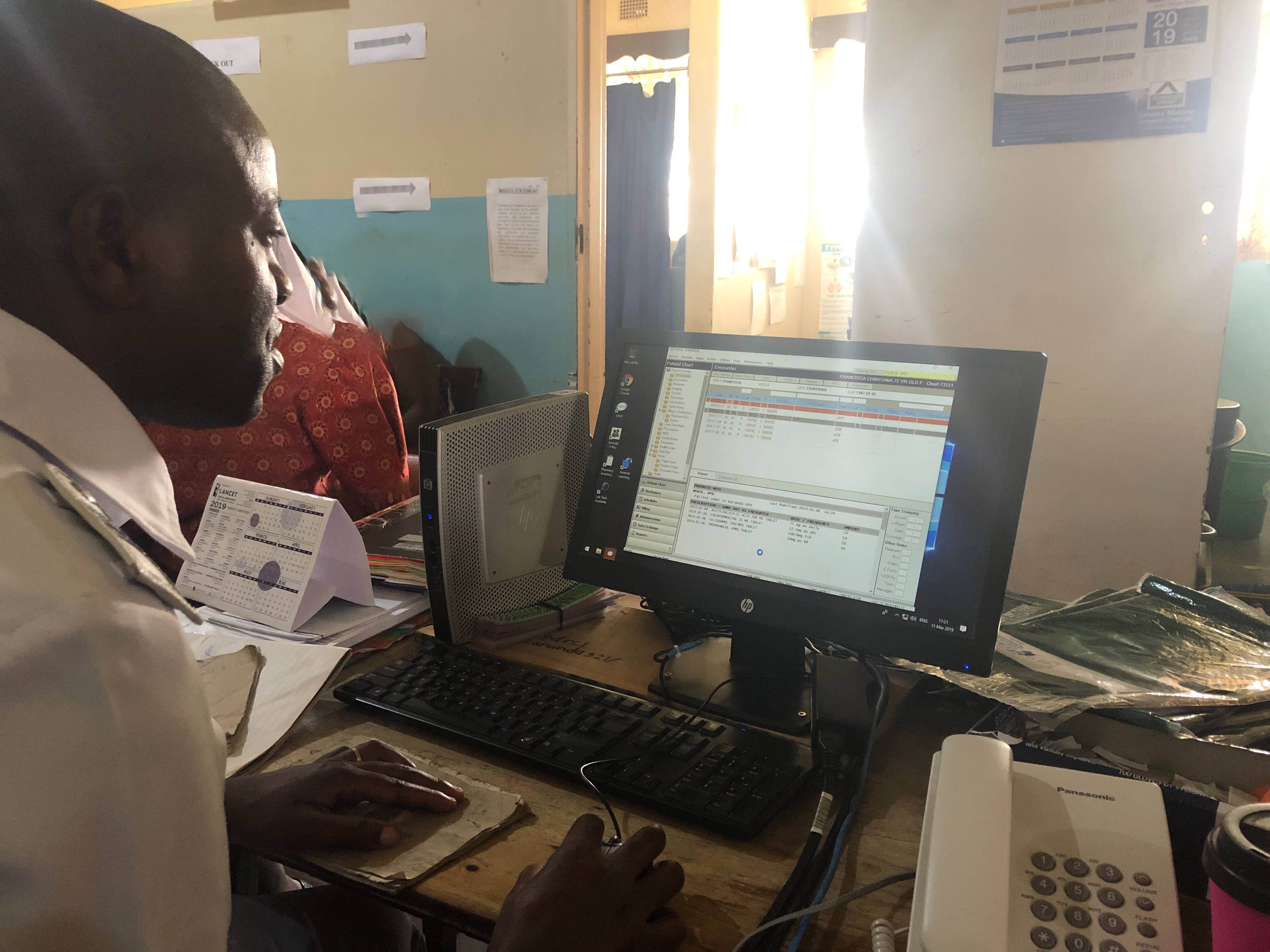 Once again the staff of Karanda have excelled. Some may recall that most of our efforts last time were to try and remove the need for the multiple accounting ledgers that were being used to record information, which some staff member then had to trawl through to extract the data required by the Zimbabwe Ministry of Health. Thus it was particularly gratifying to see that each department with MOIS was still “off book” except for the subset that the Ministry requires in a particular ledger (essentially HIV and TB). It was also incredibly gratifying to see the rapid and almost effortless way the staff were then able to extract the data they needed to (in a minute or two versus hours). Well almost effortless as there was a tiny (but extremely annoying) bug because of Canada being “Letter” and Zimbabwe being “A4” for printers. However after a few hours of: “I should remember how I fixed this!!” I did indeed remember.
Once again the staff of Karanda have excelled. Some may recall that most of our efforts last time were to try and remove the need for the multiple accounting ledgers that were being used to record information, which some staff member then had to trawl through to extract the data required by the Zimbabwe Ministry of Health. Thus it was particularly gratifying to see that each department with MOIS was still “off book” except for the subset that the Ministry requires in a particular ledger (essentially HIV and TB). It was also incredibly gratifying to see the rapid and almost effortless way the staff were then able to extract the data they needed to (in a minute or two versus hours). Well almost effortless as there was a tiny (but extremely annoying) bug because of Canada being “Letter” and Zimbabwe being “A4” for printers. However after a few hours of: “I should remember how I fixed this!!” I did indeed remember. This time of year is the rainy season and therefore “cooler” than the 40 degrees we all experienced in Oct 2016. However the fans are still required in the day and are missed when the power goes out. It does get a fraction cooler at night and I commented that this time was the first (on one night) that I actually had to pull up the bed cover. The difference in the vegetation is fascinating to see after the rain, with everything that was brown before now green. However the rains have been less than usual and the season appears to have finished early, which does not augur well for the coming dry. Already the water is being turned off at various times.
This time of year is the rainy season and therefore “cooler” than the 40 degrees we all experienced in Oct 2016. However the fans are still required in the day and are missed when the power goes out. It does get a fraction cooler at night and I commented that this time was the first (on one night) that I actually had to pull up the bed cover. The difference in the vegetation is fascinating to see after the rain, with everything that was brown before now green. However the rains have been less than usual and the season appears to have finished early, which does not augur well for the coming dry. Already the water is being turned off at various times. Amidst all these challenges to provide the basics it does seem a little irrelevant to be maintaining computers and printers and training people to use software. However the staff continue to be gracious and hard working and receptive to change. Ray always emphasizes capacity building on these trips and that is our goal. I have more “help” from Ray’s team arriving this week to expand the training, which staff have identified they need. I anticipate a productive week.
Amidst all these challenges to provide the basics it does seem a little irrelevant to be maintaining computers and printers and training people to use software. However the staff continue to be gracious and hard working and receptive to change. Ray always emphasizes capacity building on these trips and that is our goal. I have more “help” from Ray’s team arriving this week to expand the training, which staff have identified they need. I anticipate a productive week.