Sep 7 2025
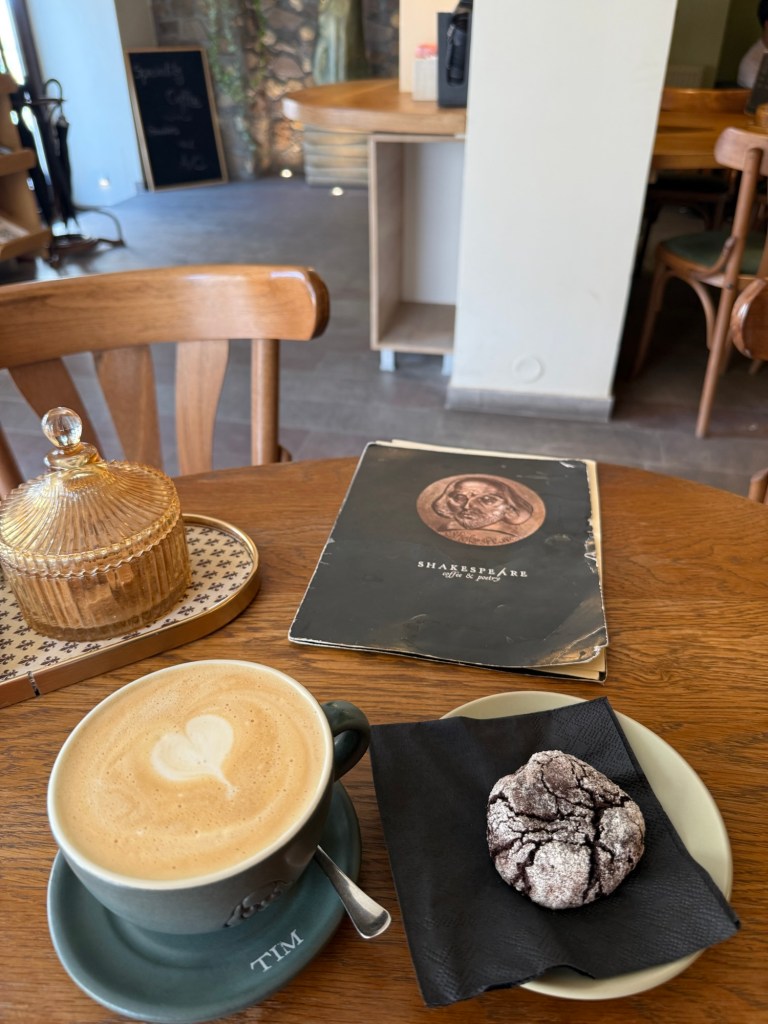
Started out early looking for the recommended cafe that Google said opened at 7. Sign said 8 on Sundays. So we wandered back up into the “old town” to one that was open. Samurai cafe. The barista lovingly crafted our drinks. So lovingly in fact that mine was quite cold by the time it reached me.. and the queue lengthened. But the view was lovely.




Fortunately the first item on the agenda was Turkish coffee. Which was hot and thick. Apparently the reading of my grounds indicated a tree. 🤷♂️


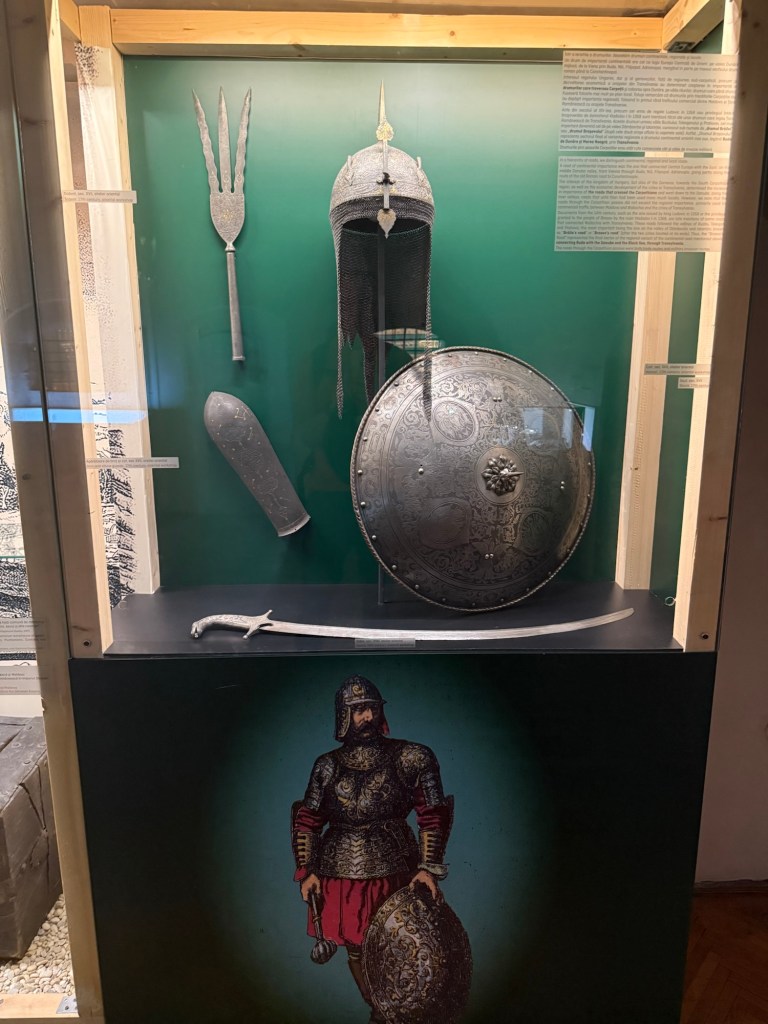
Suitably caffeinated we were deposited at the Citadel gate to go for a wander. And to spend $100 dressing up as the King and Queen of Bulgaria for photos.
For the Xmas letter.
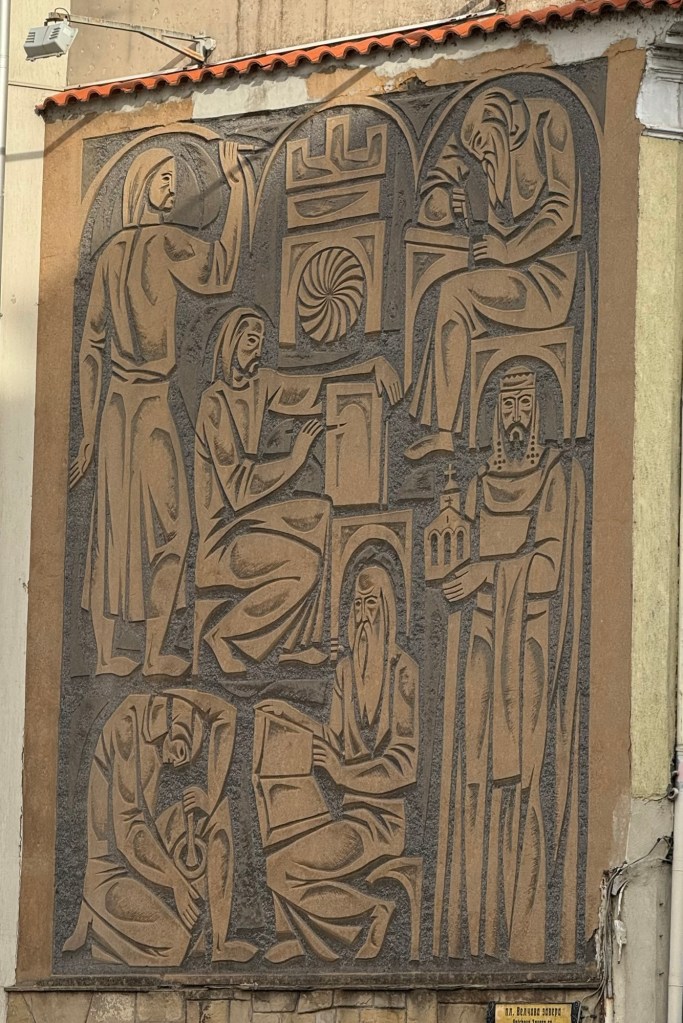
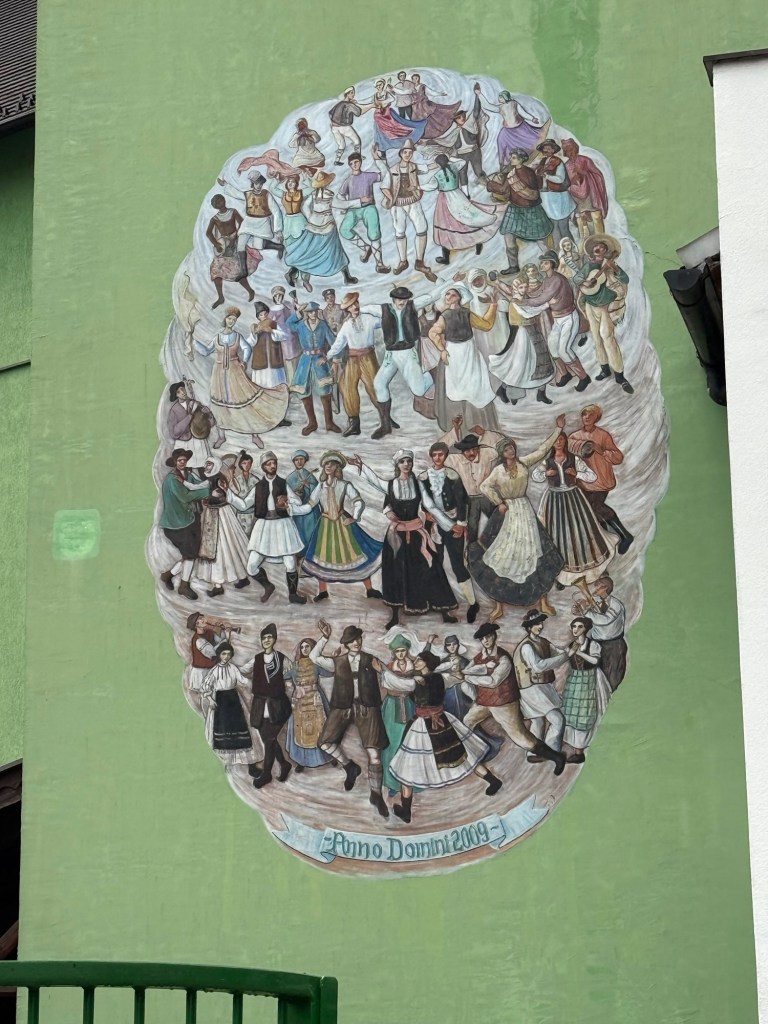
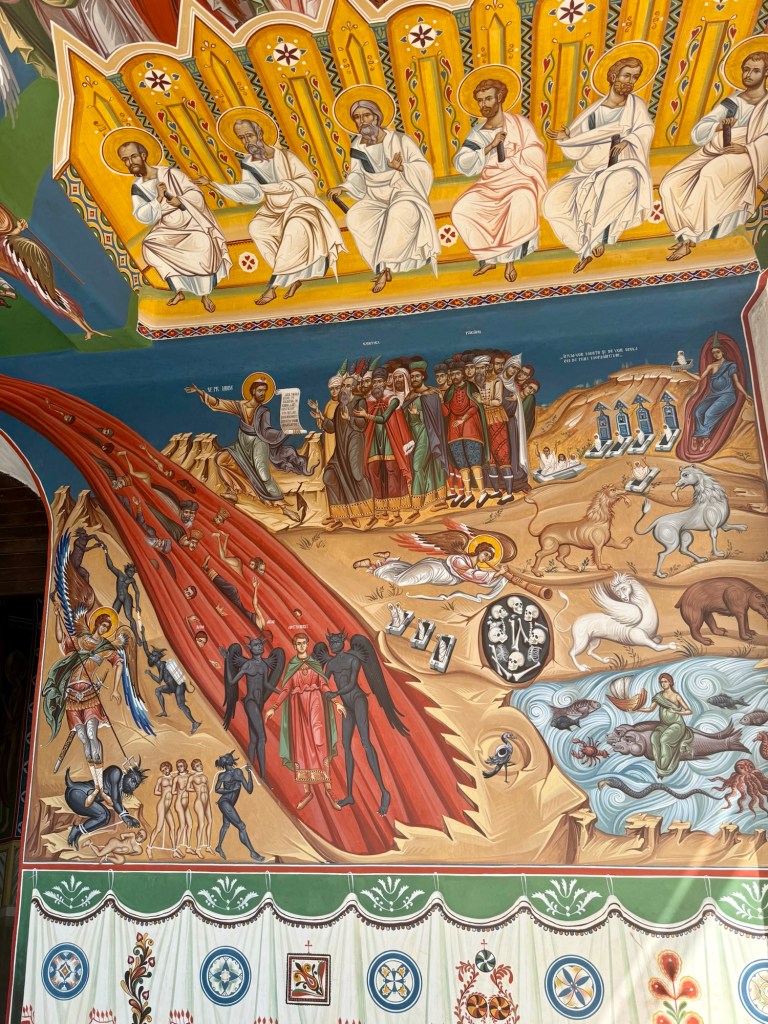
The citadel non-church was striking for its interior art work. It was never consecrated because the Queen who commissioned it also directed that it should be her visage used as that of the Madonna!





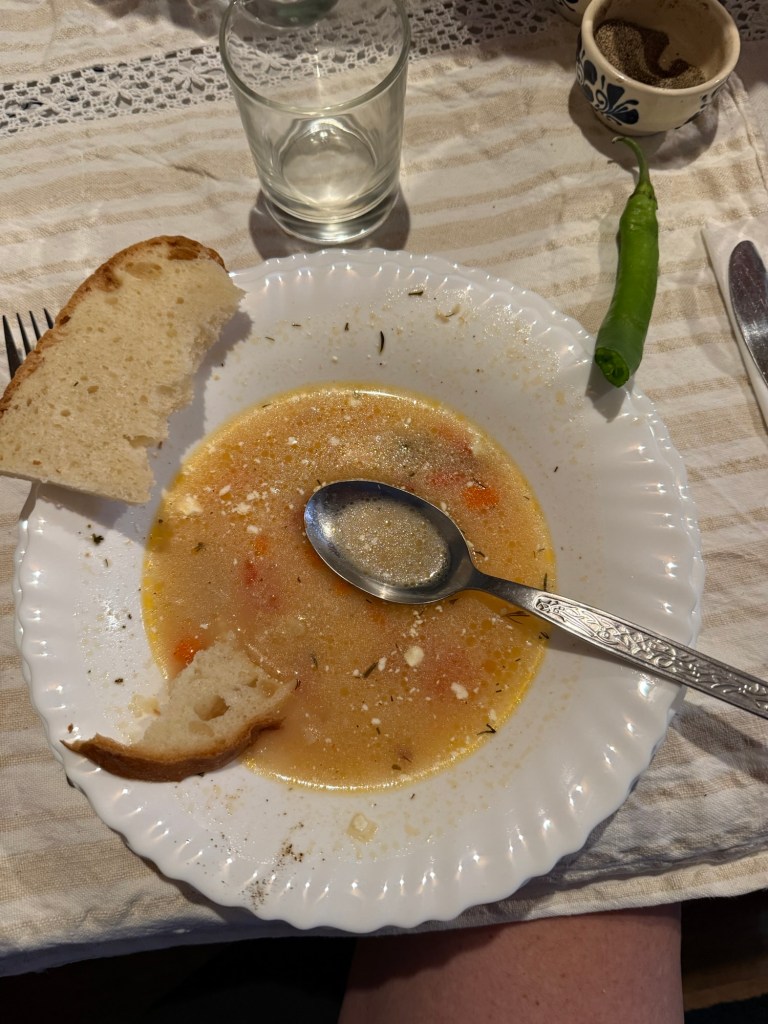
After several false lunch starts we ended up at a very authentic Italian panini place. Bath tub sized iced coffees provided a welcome tonic to the heat. Poor guy was doing it hard all on his lonesome though.
That afternoon we were determined to hike. Georgi had sent us the location link to Kartala peak. The Google review of the part beyond to the waterfall said “OK if you have nothing else to do”.
Well the whole hike was kinda that. After hotly ascending through the city we started on a dusty scrubby trail. Google wanted us to walk straight through a fence. A very obscured arrow pointed us around the McMansion to the “view point”. Except not much of the citadel could be seen as most of the view point was in the out of bounds firing range.




As it was indicated the waterfall was only a km away we thought we’d press on.
OK about described it. Quite pretty but nothing spectacular.
Fortunately the climb back up was not as bad as we anticipated. And, back on the other side of the McMansion and on our way down we discovered the best views.




Dinner was back in the pedestrian area with a nice bottle of the Gamza we’d tasted earlier. While the waiting staff dodged the cars that frequently penetrated the pedestrian zone.