This trip was not without it’s challenges but each of these came with a silver lining. Our bags missing the flight from London to Johannesburg meant I had more justification for buying additional ‘Presidential’ shirts at the airport. Difficulties in the road trip to and from Harare and Karanda made me focus on the journey. Glitches following the MOIS upgrade made me realize that local IT staff can troubleshoot many problems.
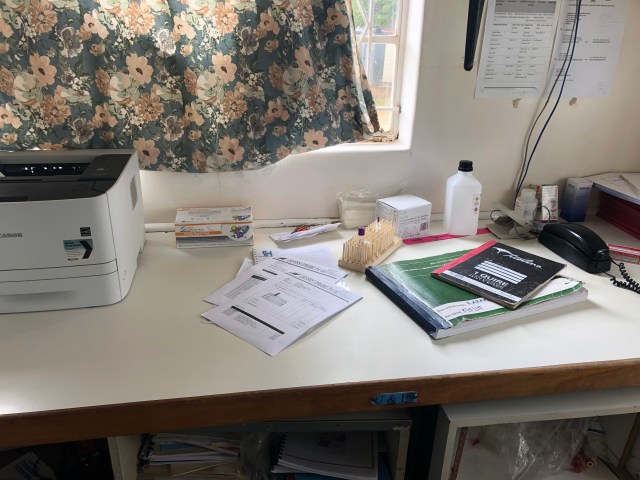
It seems I have developed somewhat of a reputation at Karanda Mission Hospital (KMH). Readers will know that one of my prime goals was to help staff at KMH free themselves from the multiple accounting registers they were using to track their work as required by the Zimbabwe Ministry of Health. Pictured above is one of the books the lab staff had gone back to using to track semen samples. My good friends in the lab were somewhat embarrassed that they were having to use a ledger book to track this information (side note: I’m not convinced that anyone from the Ministry ever looks at this information). So it was quite satisfying to quickly add a template for this data (and remind them that Zoe in the computer office has the instructions and knows how to do this:)
One of the students visiting from Toronto commented that she heard someone saying, “Here’s a ledger book (the Antenatal one) Dr Mackey doesn’t know about” to which I replied, “Oooh yes I do” (I have a picture:). I had built a flowsheet for the Antenatal Register last time I was at KMH but I am well aware that this would be a bridge too far at this time. But it’s there in case they ever end up reaching that bridge.
There was a noticeable uptick in “data integrity” while I was there. Word on the wards was that they knew I was going around and checking so staff were being a little more attentive to putting in the information. I totally understand the reticence around using the computer. For some elements, staff are having to enter the data on paper and on the computer and thus struggle to see the point. The challenge has been to impress that, if they do the data entry on the computer correctly and diligently, then they can do away with the paper and save time. Of course it is hard to alter cherished and time-honoured habits.
I did a mini presentation to the hospital staff and was truly able to say, “My work here is mostly done”. All the elements are in place for them to record the information they are required to and they are 80-90% there in the data recording. The challenge is (as always) to make the leap and leave the paper behind.

I got great help from the Drs Sean and Nicole Ebert from Vanderhoof and their son Connor in particular. He was able to do his Excel and Visial Basic wizardy so that the raw data coming out could be nicely sorted and packaged for delivery to the ministry. It was also an incredible blessing that Zoe is now employed as IT support at KMH. Whenever the “My computer’s not working” message came to the office I was able to say, “That’s Zoe’s speciality”. It was very reassuring knowing that KMH has Zoe on site to help continue the work.
Amazingly I had never previously been to eat in the “town” of Karanda. As a group we ended up visiting the same establishment twice to enjoy Zacharia’s wife’s cooking (and appreciate the work that goes into preparing sadza, the national dish). Zacharia works in the hospital CSD department and his sister-in-law, Muguti, continues to work in the pharmacy and so immediately asked how Lori was.
Not only have I experienced several figurative silver linings, but there is a literal connection with Tania’s work in wound care while we have been here. There have been some impressive advances in wound care in recent years (necessary because of the increased incidence of diabetes as well as the aging population). Silver is incorporated into some dressings for its antibacterial activity. Unfortunately these dressings are too expensive to purchase in developing countries. So even in wound care, there are great disparities between Canada and Zimbabwe. However, there were many donated dressings stored in various nooks and crannies (and scary shipping containers) that weren’t being used because there was no attached education. Tania organized the supplies and introduced and updated some practice around wound care that will have lasting benefits. She has also left behind an excellent selection of resources that will help to advance wound care at Karanda. I would again like to acknowledge the provision of prescription and non-prescription medication from Health Partners International of Canada (HPIC) and the supplies donated by uniPharm, the Vancouver-based wholesale company that Fort St John Pharmacy uses.

As with previous visits, the premier silver lining associated with all the travel hassles and the heat and the lack of sleep was re-establishing relationships and meeting new people. We are always treated with such grace and gratitude by the staff at KMH (and the people of Zimbabwe). The customs official, noticing how many Zimbabwe visas I now have in my passport asked, “When are you coming back to Zimbabwe?”.

 After a chaotic start to my travels with a 4-hour delay in Vancouver resulting in less than one hour to make a connection to Johannesburg in London (which our bags did not), I (Paul) have returned to the blog. Those who have been avidly following along will recall that this is my third sojourn to Karanda Mission Hospital, now 2 & 1/2 years since Lori, Rachelle and Thea were here. This time I linked up with the team that Dr Ray Markham puts together annually to visit Zimbabwe. It was Ray and his office staff who initially installed the electronic medical record (EMR) Medical Office Information System (MOIS) at Karanda, at the request of their administration. My first visit in 2015 was inspired by a slide presentation I heard Ray give at a conference in Montreal and he had then encouraged me to continue the MOIS install.
After a chaotic start to my travels with a 4-hour delay in Vancouver resulting in less than one hour to make a connection to Johannesburg in London (which our bags did not), I (Paul) have returned to the blog. Those who have been avidly following along will recall that this is my third sojourn to Karanda Mission Hospital, now 2 & 1/2 years since Lori, Rachelle and Thea were here. This time I linked up with the team that Dr Ray Markham puts together annually to visit Zimbabwe. It was Ray and his office staff who initially installed the electronic medical record (EMR) Medical Office Information System (MOIS) at Karanda, at the request of their administration. My first visit in 2015 was inspired by a slide presentation I heard Ray give at a conference in Montreal and he had then encouraged me to continue the MOIS install.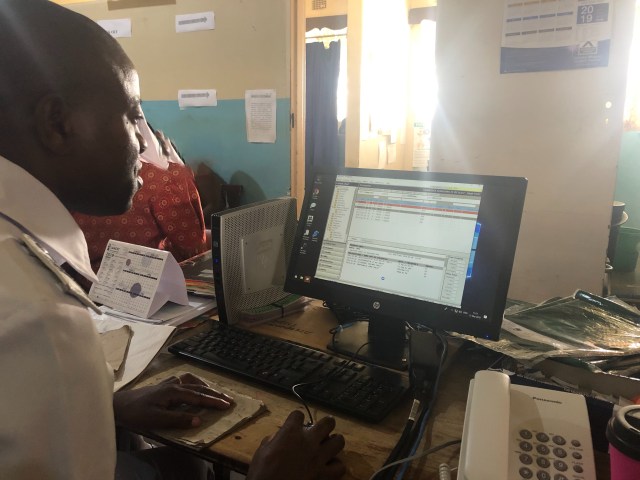 Once again the staff of Karanda have excelled. Some may recall that most of our efforts last time were to try and remove the need for the multiple accounting ledgers that were being used to record information, which some staff member then had to trawl through to extract the data required by the Zimbabwe Ministry of Health. Thus it was particularly gratifying to see that each department with MOIS was still “off book” except for the subset that the Ministry requires in a particular ledger (essentially HIV and TB). It was also incredibly gratifying to see the rapid and almost effortless way the staff were then able to extract the data they needed to (in a minute or two versus hours). Well almost effortless as there was a tiny (but extremely annoying) bug because of Canada being “Letter” and Zimbabwe being “A4” for printers. However after a few hours of: “I should remember how I fixed this!!” I did indeed remember.
Once again the staff of Karanda have excelled. Some may recall that most of our efforts last time were to try and remove the need for the multiple accounting ledgers that were being used to record information, which some staff member then had to trawl through to extract the data required by the Zimbabwe Ministry of Health. Thus it was particularly gratifying to see that each department with MOIS was still “off book” except for the subset that the Ministry requires in a particular ledger (essentially HIV and TB). It was also incredibly gratifying to see the rapid and almost effortless way the staff were then able to extract the data they needed to (in a minute or two versus hours). Well almost effortless as there was a tiny (but extremely annoying) bug because of Canada being “Letter” and Zimbabwe being “A4” for printers. However after a few hours of: “I should remember how I fixed this!!” I did indeed remember. This time of year is the rainy season and therefore “cooler” than the 40 degrees we all experienced in Oct 2016. However the fans are still required in the day and are missed when the power goes out. It does get a fraction cooler at night and I commented that this time was the first (on one night) that I actually had to pull up the bed cover. The difference in the vegetation is fascinating to see after the rain, with everything that was brown before now green. However the rains have been less than usual and the season appears to have finished early, which does not augur well for the coming dry. Already the water is being turned off at various times.
This time of year is the rainy season and therefore “cooler” than the 40 degrees we all experienced in Oct 2016. However the fans are still required in the day and are missed when the power goes out. It does get a fraction cooler at night and I commented that this time was the first (on one night) that I actually had to pull up the bed cover. The difference in the vegetation is fascinating to see after the rain, with everything that was brown before now green. However the rains have been less than usual and the season appears to have finished early, which does not augur well for the coming dry. Already the water is being turned off at various times.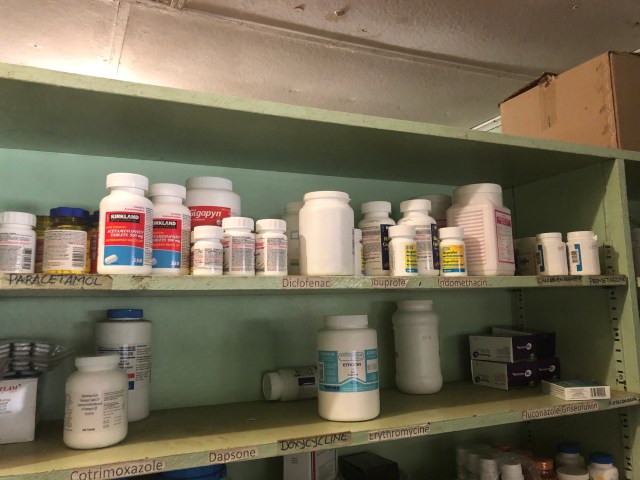 Amidst all these challenges to provide the basics it does seem a little irrelevant to be maintaining computers and printers and training people to use software. However the staff continue to be gracious and hard working and receptive to change. Ray always emphasizes capacity building on these trips and that is our goal. I have more “help” from Ray’s team arriving this week to expand the training, which staff have identified they need. I anticipate a productive week.
Amidst all these challenges to provide the basics it does seem a little irrelevant to be maintaining computers and printers and training people to use software. However the staff continue to be gracious and hard working and receptive to change. Ray always emphasizes capacity building on these trips and that is our goal. I have more “help” from Ray’s team arriving this week to expand the training, which staff have identified they need. I anticipate a productive week.